Medically reviewed by the Know Your Surgery Editorial Team. Last reviewed: May 2026.
Once mastectomy is decided, most patients want to know exactly what happens next. Mastectomy in the United States follows established pathways that vary by type and by whether reconstruction is performed at the same time. This article walks through preparation, the surgery step by step, anesthesia, and what recovery typically looks like over the days, weeks, and months that follow.
If you have not yet read about why mastectomy may be needed, our causes, diagnosis, and decision article covers how the decision is made.
Preparing for Mastectomy
Mastectomy is usually scheduled days to a few weeks in advance. The surgical team typically:
- Reviews recent imaging and biopsy results
- Reviews medications, including blood thinners and hormonal medications
- Orders pre-operative blood and (sometimes) cardiac tests
- Asks the patient to fast the night before surgery
- Coordinates with the plastic surgery team if reconstruction is planned
- Performs an anesthesia consultation
- Discusses informed consent, including risks and recovery
- Provides educational materials on drain care, post-op exercises, and emotional support resources
The patient arrives at the hospital, changes into a gown, and is prepared for the operating room.
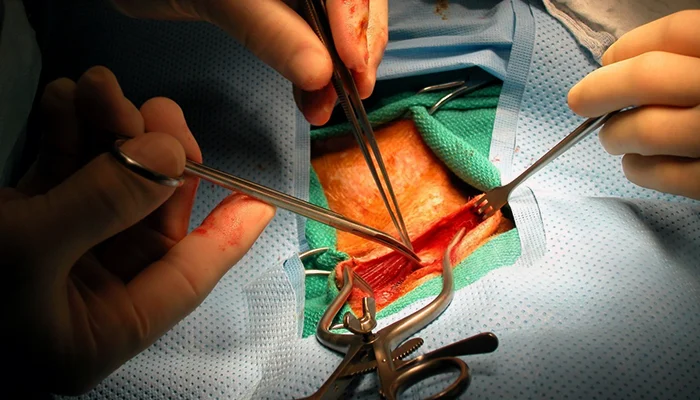
Total (Simple) Mastectomy Step by Step
A total mastectomy typically takes 1.5 to 2.5 hours, longer if combined with sentinel lymph node biopsy or reconstruction.
- General anesthesia is administered.
- The chest is cleaned with antiseptic and draped sterile.
- A horizontal or oval incision is made across the breast, designed to allow safe cancer removal and good cosmetic outcome.
- The breast tissue is carefully separated from the overlying skin and the underlying chest wall muscles.
- The breast tissue, nipple, and areola are removed. The chest wall muscles are preserved.
- Sentinel lymph node biopsy may be performed at the same time if planned (a small number of underarm lymph nodes are removed and tested).
- A drain (or two) is placed to remove fluid that collects after surgery. The drain exits through a small opening in the skin and connects to a soft bulb.
- The skin is closed with sutures, often absorbable.
- Sterile dressings are applied.
If immediate reconstruction is planned, the plastic surgeon takes over to begin the reconstruction. If not, the patient is moved to the recovery area.
Modified Radical Mastectomy Step by Step
A modified radical mastectomy adds removal of most underarm lymph nodes (axillary lymph node dissection). The procedure typically takes 2 to 3 hours.
- Steps 1 to 5 as in total mastectomy.
- The dissection extends into the underarm, where the surgeon carefully removes most of the level I and level II lymph nodes.
- Drains are placed in both the chest and underarm.
- Closure as above.
Removing more lymph nodes raises the risk of long-term arm swelling (lymphedema), so this procedure is reserved for cases where less extensive node surgery is not appropriate.
Skin-Sparing and Nipple-Sparing Mastectomy
These approaches preserve more of the breast skin envelope (and, in nipple-sparing, the nipple-areola complex) to allow better reconstruction outcomes. The procedure usually takes 2 to 4 hours, longer with reconstruction.
- The breast tissue is removed through a small incision (often around the areola or under the breast fold) while preserving the skin.
- The breast tissue is carefully separated from the skin.
- In nipple-sparing, tissue beneath the nipple is sampled and tested while the nipple-areola complex is preserved.
- Reconstruction is typically performed at the same time.
Skin-sparing and nipple-sparing techniques require careful patient selection based on tumor location, size, and biology.
Reconstruction Options
Reconstruction can be performed at the time of mastectomy (immediate) or later (delayed). The main options are:
Implant-based reconstruction. A tissue expander or implant is placed under the chest muscle or above the muscle. May be done in stages.
Autologous (flap) reconstruction. Uses the patient’s own tissue from the abdomen (DIEP flap, TRAM flap), back (latissimus flap), or thigh.
No reconstruction. Some patients choose to remain flat or use external prosthetics.
The plastic surgery team discusses options in detail before surgery.
Anesthesia for Mastectomy
The standard is general anesthesia. The anesthesia team monitors closely throughout, including breathing, heart rhythm, and oxygen. Modern anesthesia is highly safe; the team accounts for any heart, lung, or other medical conditions in the plan.
Some centers offer regional anesthesia (paravertebral block or PECS block) to improve post-op pain control.
What Happens Right After Surgery

After surgery, the patient is moved to a recovery area for monitoring of vital signs, pain, and the surgical site. Anesthesia gradually wears off over 30 to 90 minutes. Common features include:
- Soreness and tightness across the chest
- A drain (or two), which is checked and started on a recording schedule
- A surgical bra or compression garment
- Mild nausea from anesthesia (usually transient)
- Limited arm movement on the surgical side initially
Most patients are admitted overnight (or longer for reconstruction). Pain is controlled with a combination of acetaminophen, NSAIDs (if approved), and a short course of opioid medication if needed.
Recovery Timeline
Recovery depends on the procedure and whether reconstruction was done.
Day 1. Pain control. Walking is encouraged early to reduce blood-clot risk. Drain education begins.
Days 1 to 2 in the hospital. Diet advances. Drain output is recorded. The patient learns drain care, dressing care, and gentle arm exercises.
Week 1 at home. Rest, drain management, gentle movement. Most patients shower (with drain protection) within a few days.
Weeks 1 to 2. Drain removal at follow-up visit when output is low enough (typically 10 to 14 days). Sutures and dressings are checked.
Weeks 2 to 4. Many patients return to office work for simple mastectomy without reconstruction. Activity gradually expands. Driving usually resumes once off prescription pain medication.
Weeks 4 to 6. Most patients return to most normal activities. Heavier lifting and full exercise are restricted longer.
Months 2 to 6. Continued recovery for patients with reconstruction. Additional surgeries may be planned (such as expander-to-implant exchange or nipple reconstruction).
These timelines are general. Patients with reconstruction, complications, or additional treatments may take longer. Always follow your surgical team’s specific instructions.
Drain Care
A drain is one of the most universal parts of mastectomy recovery. Care includes:
- Empty the bulb as instructed (often two to three times daily)
- Record the volume and color of fluid each time
- Strip the tubing gently to prevent clogs (per the team’s instructions)
- Keep the drain site clean and dry
- Watch for redness, warmth, or pus at the exit site
The drain is removed at the follow-up visit when output drops to a defined threshold. Removal is usually quick and not very painful.
Pain Management
Pain after mastectomy is typically controlled with:
- Scheduled doses of acetaminophen
- NSAIDs (if approved)
- A short course of stronger pain medication if needed
- Cold compresses
- Muscle relaxants for certain patients
- A regional anesthesia block placed at surgery (at some centers)
Severe pain that is worsening, fever, or signs of infection should prompt immediate contact with the surgical team.
Activity Restrictions and Common-Sense Care
In the first 1 to 6 weeks, the chest and underarm are healing. Common restrictions include:
- No heavy lifting (typically over 5 to 10 pounds initially) for several weeks
- No driving until off prescription pain medication and able to react safely
- No raising the arm overhead beyond gentle stretches initially
- No vigorous exercise until cleared
- No swimming or hot tubs until incisions and drains are healed
- Sleep with extra pillows for support
A physical therapist may guide gentle range-of-motion exercises to prevent stiffness.
Detailed warning signs are covered in our FAQs and statistics article.
Lymphedema Prevention
If lymph nodes were removed (especially with axillary dissection), there is a long-term risk of arm swelling (lymphedema). Steps to reduce risk include:
- Gentle exercises as recommended by physical therapy
- Avoiding blood draws or blood pressure measurements in the affected arm when possible
- Skin care to reduce infection risk
- Compression garments if recommended
Specialized lymphedema therapists can help if swelling develops.
Follow-Up Appointments
A typical follow-up schedule includes:
- Phone or in-person check during the first week
- Office visit at 1 to 2 weeks for drain removal and wound check
- Pathology review meeting to discuss results and any additional treatment
- Coordination with medical oncology, radiation oncology, or plastic surgery as needed
- Lifelong follow-up with breast surveillance and survivorship care
Rehabilitation and Long-Term Outlook

Many patients benefit from rehabilitation:
- Physical therapy for shoulder mobility and strength
- Occupational therapy for return to daily activities
- Lymphedema therapy if needed
- Counseling and support groups for emotional adjustment
- Survivorship clinics for long-term care
Long-term outlook depends on cancer stage, type, and additional treatments. Many women live full, active lives after mastectomy. Survivorship plans address surveillance, side effect management, and ongoing health.
Continue Reading the Mastectomy Cluster
- Mastectomy: Overview, Types, and What to Expect
- Mastectomy: Causes, Diagnosis, and When to Consider Surgery
- Mastectomy: FAQs, Statistics, and Patient Stories
Sources
- American Cancer Society (ACS). Mastectomy: procedure and recovery. https://www.cancer.org/cancer/types/breast-cancer/treatment/surgery-for-breast-cancer/mastectomy.html
- National Cancer Institute (NCI). Breast cancer treatment. https://www.cancer.gov/types/breast/patient/breast-treatment-pdq
- Mayo Clinic. Mastectomy: what to expect. https://www.mayoclinic.org/tests-procedures/mastectomy/about/pac-20384879
- Cleveland Clinic. Mastectomy: procedure and recovery. https://my.clevelandclinic.org/health/treatments/8330-mastectomy
- American Society of Plastic Surgeons (ASPS). Breast reconstruction options. https://www.plasticsurgery.org/reconstructive-procedures/breast-reconstruction
Medical Disclaimer
The information in this article is for general education and is not a substitute for professional medical advice, diagnosis, or treatment. Always consult your surgical team with questions about your procedure, medications, or recovery.